Courbes cognitives QuoCo
L'outil développé pour aider le clinicien à suivre la cognition de ses patients âgés, à la manière de mesures morphométriques des courbes de croissance pédiatriques.
À propos de QuoCo
QuoCo MMSE
Contexte
Il est d'un commun accord de considérer que la cognition diminue à mesure que l'âge d'un individu augmente. Par contre, quel est le déclin cognitif normal? Comment peut-on départager l'apparition d'une maladie neurologique du seul impact de l'âge?
Nous sommes fiers de présenter QuoCo, l'outil développé pour aider le clinicien à répondre à ces questions de façon simple et efficace avec des courbes de percentile.
D'où viennent les courbes?
Développé par notre équipe interdisciplinaire de chercheurs, QuoCo a été construit à partir des résultats de la fameuse étude "Canadian Study of Health and Aging". Nos courbes cognitives ont été validées avec plus de 8 000 entrées de la banque de données américaine National Alzheimer’s Coordinating Center' UDS. Ces courbes permettent de suivre le score QuoCo des patients à la manière de mesures morphométriques des courbes de croissance pédiatriques.
Nos données ont été publiées dans la prestigieuse revue CMAJ. Notre article est disponible en ligne et en version PDF.
De quoi avez-vous besoin pour calculer le QuoCo?
Vous n'avez besoin que de l'âge du patient, de son nombre d'années de scolarité et de son(ses) score(s) au MMSE (Idéalement avec "MONDE" épelé à l'envers). L'outil permet d'estimer l'état de la cognition du patient avec un seul ou plusieurs scores MMSE. L'outil n'est pas conçu pour suivre des patients dont le diagnostic de trouble neurocognitif majeur (démence) est déjà posé. L'idéal est d'avoir un score MMSE de base (baseline) lorsque le patient est plus jeune (65-70 ans) et clairement intact au plan cognitif.
Les calculs
Il vous suffit ensuite de calculer le QuoCo et l'Âge standardisé (AS).
Placez ensuite les résultats du QuoCo et de l'Âge standardisé sur les courbes cognitives (CC).
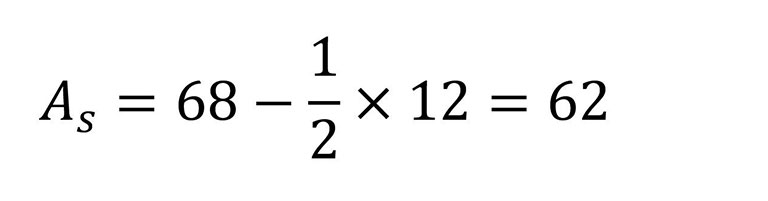
À noter que l'âge réel minimal doit être de 65 ans et que la scolarité est plafonnée à 14 ans lors des calculs. Donc, pour n'importe quelle scolarité plus grande que 14 ans, on retranche 7.
L'âge et la scolarité sont toujours représentés en années.
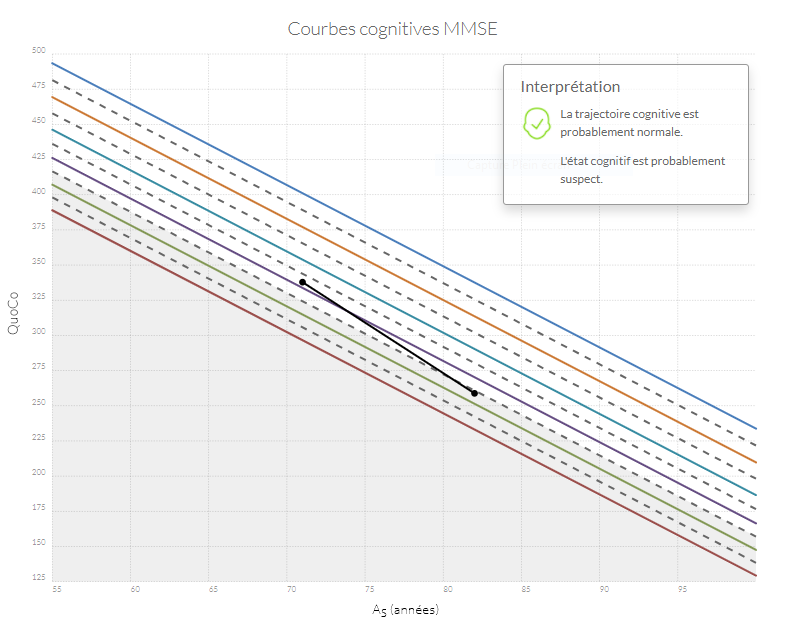
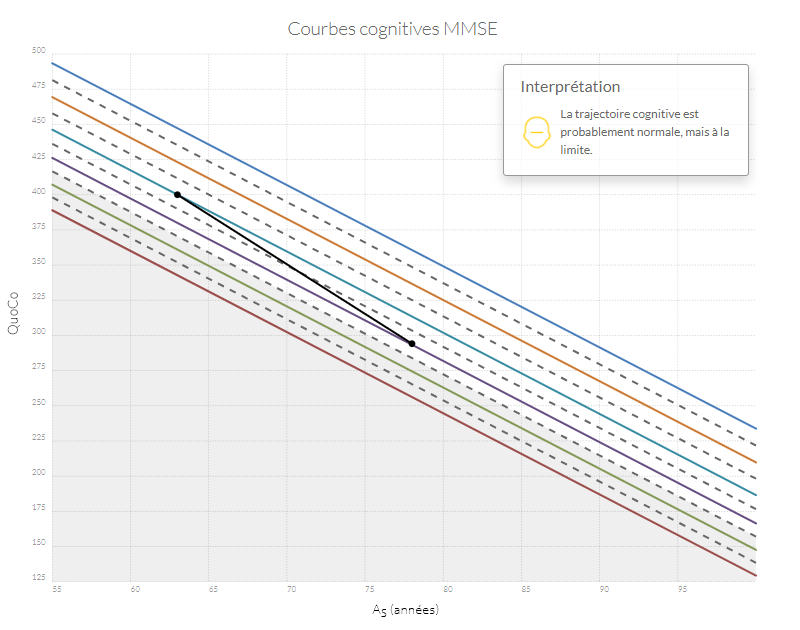
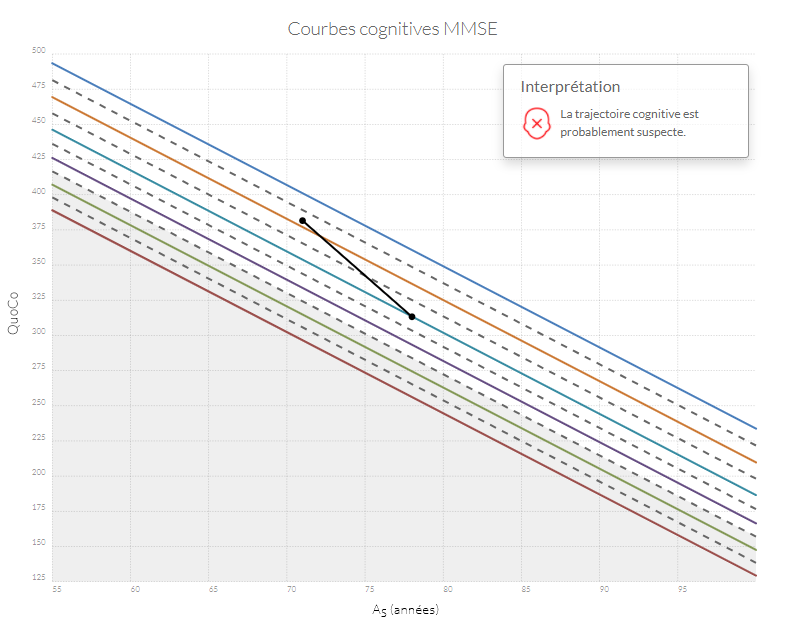
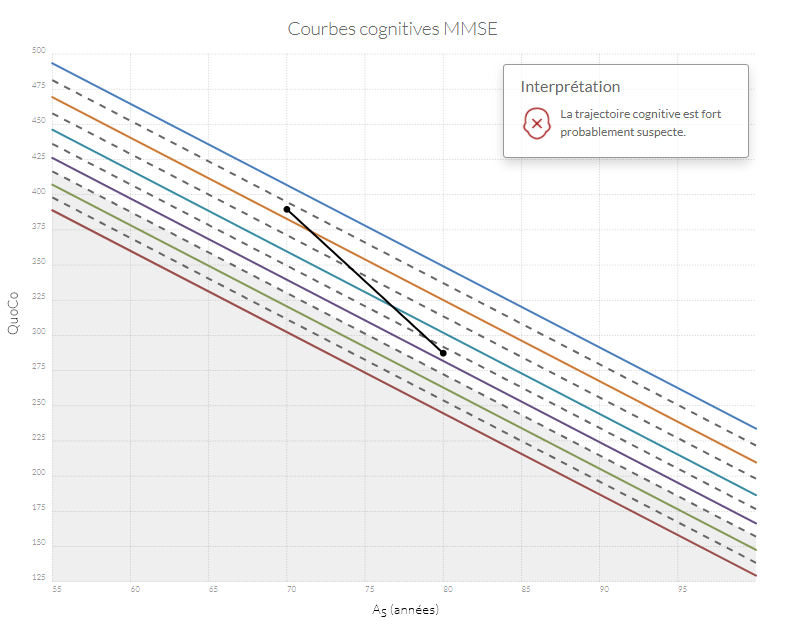
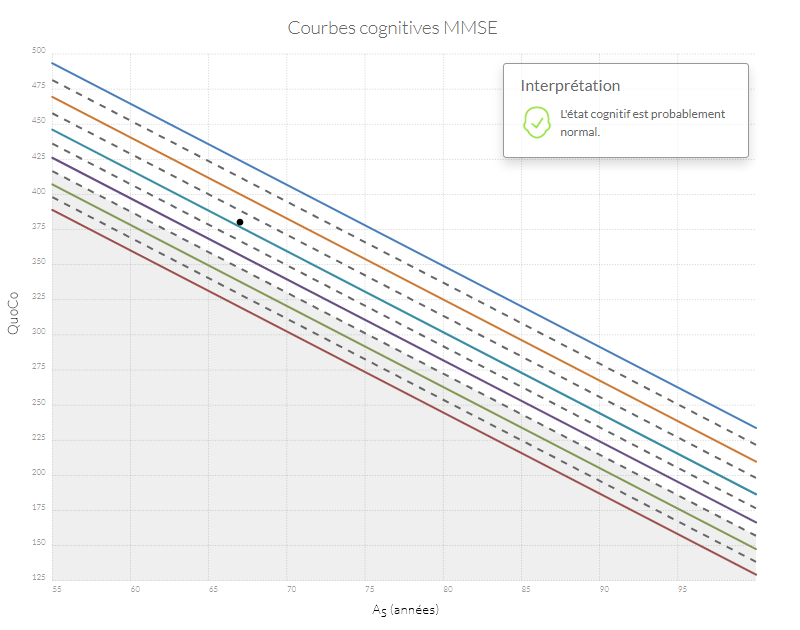
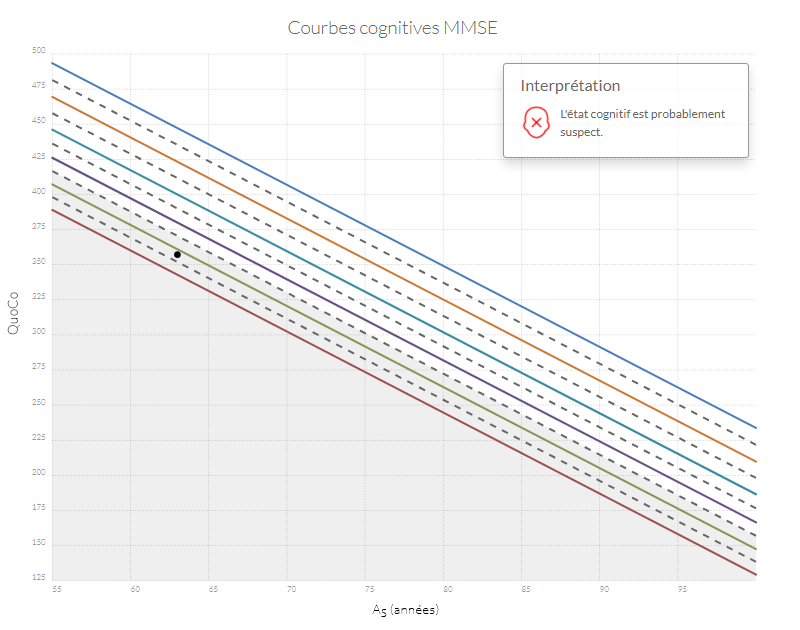
Interprétation des données
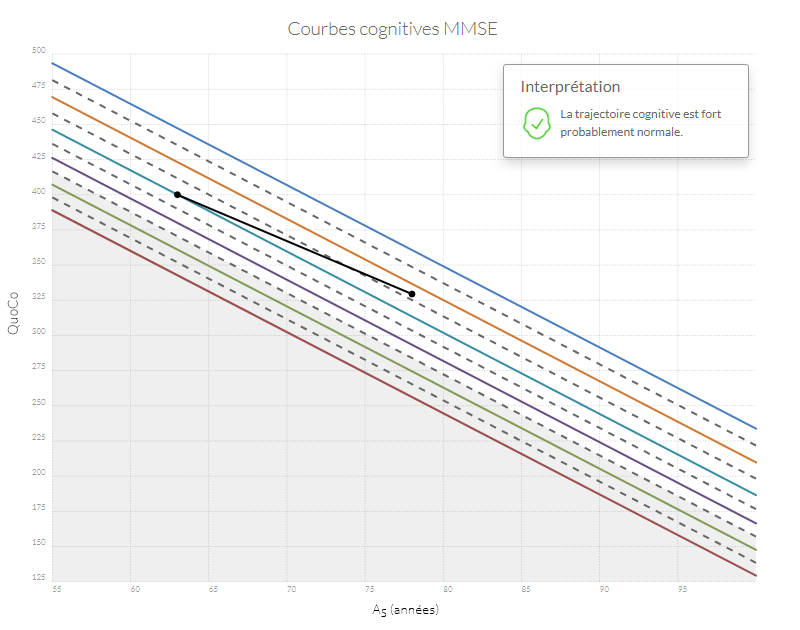
Si n'importe quel point se retrouve dans la zone grise, l'état cognitif du patient est probablement anormal. Si la trajectoire entre le point d'origine (baseline) et le point le plus récent diminue de plus d'un intervalle (correspondant à l'équivalent de l'espace entre deux lignes) le patient a probablement un déclin cognitif anormal.
Voici l'exemple d'une femme agée qui possède 12 années de scolarité :
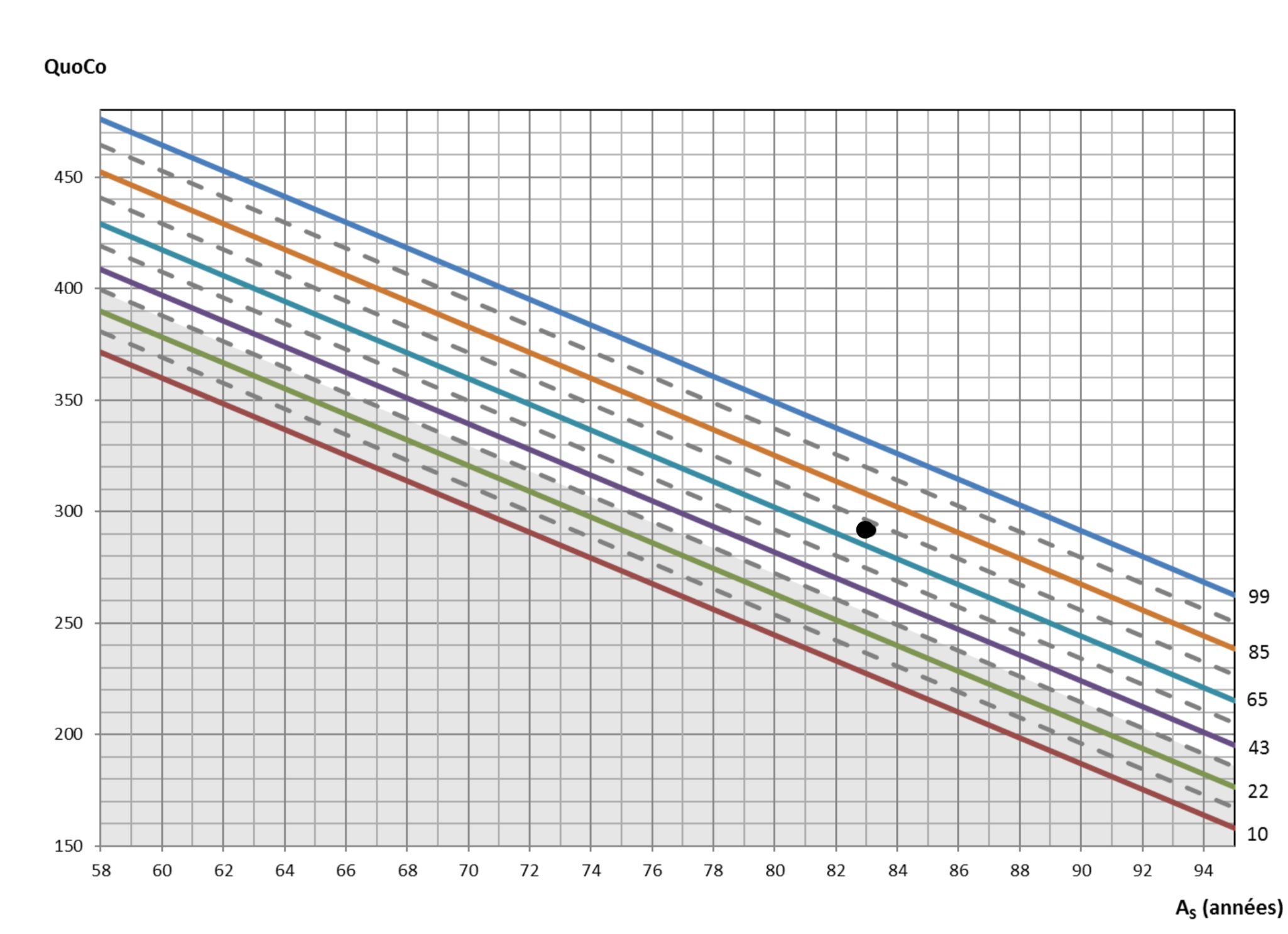
À 89 ans, elle a obtenu un score de 26 sur 30 au MMSE.
En plaçant son résultat sur les courbes cognitives, on obtient :
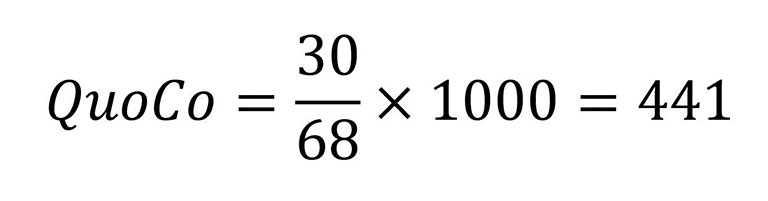
À 68 ans, elle a obtenu un score de 30 sur 30 au MMSE.
On peut maintenant voir sa trajectoire cognitive au fil du temps :
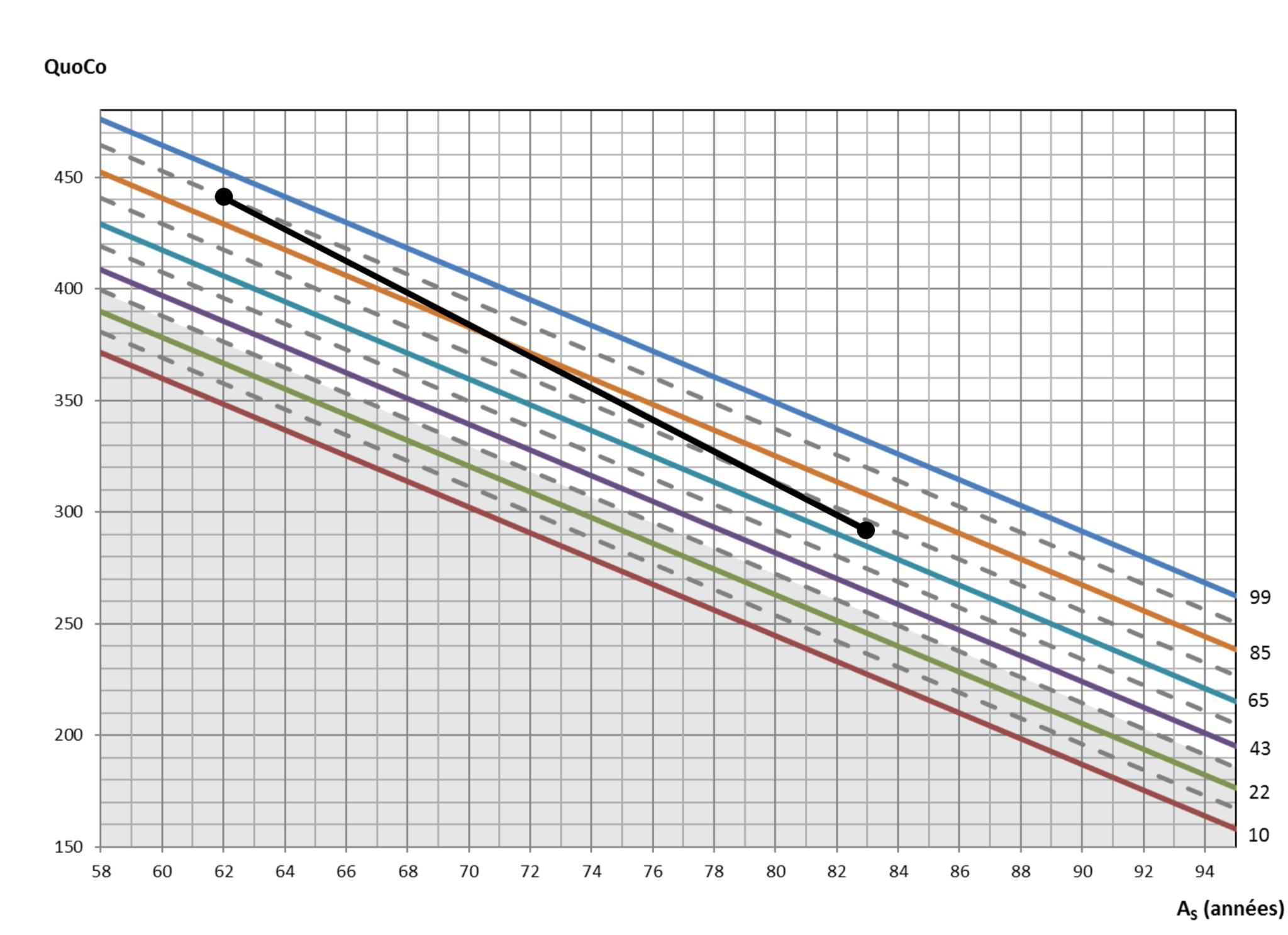
Ce cas montre donc un déclin anormal, car le QuoCo descend de plus d'un intervalle.
Exemples de trajectoires cognitives
Tutoriels & FAQ
Visionnez le tutoriel pour apprendre en détails comment utiliser les Courbes Cognitives MMSE :
OU
Pour plus de réponses, visitez notre section Foire aux questions - MMSE
Q : Quelle est la différence entre « l’état cognitif » et la « trajectoire cognitive »?
R : L’état cognitif est représenté sur les courbes par la position d’un point à un moment précis sans tenir compte de l’évolution dans le temps. Un patient a un état cognitif suspect si le point se situe dans la zone grise. La trajectoire cognitive du patient correspond à la ligne joignant un point que l’on considère comme référence (baseline) et le dernier point obtenu pour ce patient (point actuel).
Q : Qu’est-ce qu’un intervalle?
R : Un intervalle correspond à la zone entre deux lignes pleines ou deux lignes pointillées sur les courbes vers le bas. Si un point est entre 2 lignes, le clinicien n’a qu’à calculer l’équivalent d’unintervalle vers le bas selon le percentile le plus près.
Q : Quand la trajectoire cognitive est-elle suspecte?
R : C’est lorsque la trajectoire d’un individu passe à travers au moins un intervalle complet à partir de son point de référence (baseline). Puisque ce point n’est pas nécessairement directement sur une ligne, il faut considérer l’équivalent de l’intervalle le plus proche du baseline. (Voir notre tutoriel vidéo pour plus d'informations)
Q : Pourquoi dois-je multiplier par 1000 pour avoir le QuoCo?
R : C'est principalement pour éliminer les décimales. Aussi, un résultat sur 1000 évite la confusion avec d'autres tests sur 100 comme le 3MS par exemple.
Q : Mon patient a 20 ans de scolarité. Pourquoi je ne retranche pas 10 de l'âge réel pour obtenir son âge standardisé?
R : La valeur maximum de la scolarité est fixée à 14 ans. Toutes les scolarités supérieures ne retranchent quand même que 7 ans. Les courbes cognitives ont été construites à partir d'une vaste banque de patients normaux desquels nous avons le MMSE, l'âge et la scolarité. Nos analyses ont démontré que le MMSE n'est pas plus influencé favorablement au delà de 14 ans de scolarité.
Q : Je n'ai pas de MMSE de base (baseline) pour mon patient. Est-ce que je peux utiliser QuoCo?
R : Oui. Si vous avez un MMSE antérieur au moment où le patient n'avait pas de diagnostic de TNC majeur (démence), vous pouvez l'utiliser comme point de référence avec le MMSE actuel. Si vous avez seulement le MMSE actuel, la zone grise (cutoff) vous permet quand même d'évaluer la performance du patient au test.
Q : Doit-on toujours prendre le point initial comme baseline?
R : Non. Il est possible de prendre un autre point comme baseline. Par exemple, si un patient remonte sur les courbes cognitives, certains préféreront définir le point le plus haut atteint par le patient comme baseline. Cette dernière notion est actuellement à l’étude par notre équipe.
Q : Le point que je tente de placer n'entre pas dans le graphique. Pourquoi?
R : Vous avez probablement un patient dont l'âge réel n'est pas dans les âges étudiés pour créer les courbes cognitives (c'est à dire entre 65 et 95 ans). Un patient plus jeune que 58 ans d'âge standardisé ne peut pas être placé sur les courbes. Avez-vous bien tenu compte du maximum de 7 comme soustraction sur l'âge?
Q : Le score QuoCo fait en sorte que le point est au dessus des courbes. Que se passe-t-il?
R : Le résultat de votre patient est exceptionnellement bon et diverge plus haut que le meilleur percentile obtenu par l'analyse statistique. Tout va bien.
Q : La trajectoire monte au lieu de descendre. Qu'est-ce que ça veut dire?
R : L'évolution des performances aux tests du patient est supérieure à ce qui est normalement attendu. Sa trajectoire est donc fort probablement normale.
Q : Le déclin du score QuoCo de mon patient représente presque directement un intervalle. C'est donc limite. C'est normal ou non?
R : Nos analyses ont permis d'établir que dès qu'un intervalle est franchi, la trajectoire est probablement suspecte. Par contre, plus le déclin est grand, plus la trajectoire est suspecte. Lorsque la trajectoire arrive directement sur l'autre percentile, elle est théoriquement encore acceptable, mais le jugement du clinicien prévaut toujours.
Q : Le premier point était dans le gris (probablement suspect), mais le patient n'était pas atteint d'un TNC majeur (démence). Puis-je alors suivre sa trajectoire?
R : Oui, si vous êtes confiant que le score QuoCo précédent représentait une performance normale. Les lignes percentile dans la zone grise vous guideront à estimer la trajectoire attendue.
Q : Dois-je utiliser le score de MMSE avec « MONDE à l'envers » ou « 100‑7 »?
R : Les courbes cognitives ont été développées à partir des scores de MMSE avec « MONDE à l'envers ».
Q : Pourquoi les lignes de percentile sont-elles plus rapprochées vers le bas?
R : C'est parce que les espaces entre les lignes de percentile ont été déterminés pour départager au mieux la trajectoire normale par rapport à celle des gens qui développent un TNC majeur (démence). Pour les percentiles inférieurs, le déclin possible est moindre puisque les résultats sont déjà plus faibles.
Q : Est-ce que je peux utiliser le MoCA sur les courbes cognitives?
R : Non. Pour l'instant, c'est uniquement le MMSE qui a été étudié.
Visionnez le tutoriel pour apprendre en détails comment utiliser les Courbes Cognitives MoCA :
Équipe QuoCo

Patrick Bernier
MD/PhD/CCMF Concepteur et co-développeur de l'outil
Chef de projet

Christian Gourdeau
MSc ing physique Co-développeur de l'outil
Leader des calculs, analyse et modélisation

Robert Laforce Jr
MD/PhD/FRCP Chef de la recherche et publication

Pierre-Hugues Carmichael
Biostatisticien et responsable de la validation
Jean-Pierre Beauchemin
MD Conseiller clinique et scientifique